
Study population
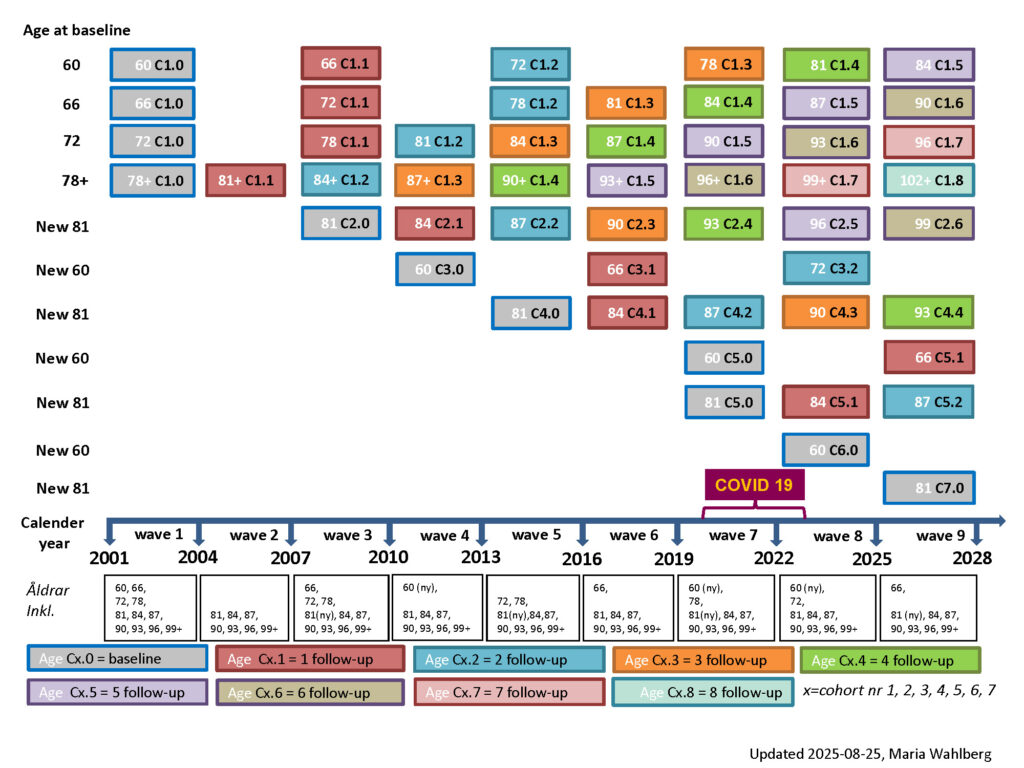
The study populations of SNAC-K consist of individuals aged 60+ and living at home or in institutions on the island of Kungsholmen. The study used stratified sampling; the Kungsholmen population was first stratified by age, and then a random sample was selected from each age group. In total, eleven age cohorts were chosen with two different age intervals: 6-year intervals in the younger cohorts (60, 66, 72 and 78 years), and 3-years intervals in the older cohorts (81, 84, 87, 90, 93, 96 and 99+ years). Follow-up is performed every 6 years for younger cohorts (60–78 years) and every 3 years for older cohorts (age 78+ years). The baseline data collection was conducted during 2001-2004. The figure below shows the timetable for data collection in SNAC-K.
The sample sizes were determined originally by the national SNAC project. However, in SNAC-K we chose to oversample the 3 youngest age groups to have a sufficiently large sample size for longitudinal analyses. A final total of 3363 persons participated at baseline in SNAC-K.
Baseline data collection
The baseline data collection includes information on present status and past events. The information has been collected through interviews, clinical examinations, and testing. All staff (nurses, psychologists, and physicians) has been trained for data collection. Each subject has been examined for six hours on average; two hours for the social interview and the assessment of physical functioning (performed by a nurse); two hours for clinical examination, including geriatric, neurological and psychiatric assessment (performed by a physician); and two hours for cognitive assessment (performed by a psychologist).
Assessment and clinical examination
Five different protocols have been completed and implemented:
1. The nurse questionnaire including a social interview and assessment of physical functioning
2. The clinical form and diagnostic conclusions for the medical examination
3. The psychological test battery
4. The informant interview, when the subject was unable to answer
5. A self-administered questionnaire

Test of grip strength. Photo: Stefan Zimmerman
The Nurse Interview assesses: 1) Demographic data; 2) Living arrangement: type, organization, and changes; 3) Education, and current and past life occupational history (classification according to the Nordic Occupational Coding); 4) Current and past socio-economic status of the subject and the family; 5) Life habits including past and present alcohol consumption and smoking (type, quantity, and length of exposure); 6) Physical functioning with information collected on ADL, IADL, motility and strength, sensory functions (most of commonly used scales are fulfilled), and with observational tests concerning hand strength, walking speed, and balance; 9) Use of medical and social facilities; and finally 10) Formal and informal care received and provided.

Blood pressure control. Photo: Stefan Zimmerman
The Clinical Form includes 1) Family and past clinical history; 2) Current and past use of drugs; 3) Geriatric examination: general status, heart with ECG and lung function, blood pressure measurements, and symptoms including pain; 4) Neurological examination including also assessment of episodic and semantic memory, language, abstract thinking, praxis, visuospatial ability, gnosis and frontal lobe tests; 5) Dementia severity according to the Clinical Dementia Rating scale; 5) Psychiatric examination including two scales: the Comprehensive Psychopathological Rating Scale and the Neuropsychiatric Inventory; 6) Laboratory tests for all subjects; and 7) diagnostic conclusions according to standardized criteria.
The Psychological Test Battery assesses five major cognitive domains: 1) Episodic memory: item and source memory; recollection and familiarity; recall and recognition; 2) Mental tempo: motor and perceptual speed; 3) Executive functioning: trial making test and verbal fluency, 4) Spatial function: mental rotation, 5) semantic memory: general knowledge; metacognitive judgments. The task battery has been prepared in order to optimize the possibility of identifying individuals at risk for developing different disorders with cognitive repercussions (e.g., dementia, depression) at the earliest possible time.
The Self-Administered Questionnaire includes 1) Social network: instrumental and emotional support, social anchorage, social participation and control; 2) Leisure activities including physical, recreational and productive activities (current and past); 3) Nutritional assessment; 4) Health related life quality (Short Form 12 Health Survey); 5) Neugarten Life Satisfaction Index; 6) Well-being assessed by PANAS; and 7) Ware´s Health Perceptions Questionnaire.
The whole examination is 5-6 hours long, with almost two hours for each part administered by the nurse, the physician and the psychologist, respectively.
Follow-up data collection
As noted, the follow-up interval is six years long for the younger age cohorts, and three years for the older age cohorts. Each birth cohort will be re-examined when subjects reach the age of the following age group. During the follow- up intervals, medical events of all subjects will be registered through linkage with primary care registry (when available) and hospital registry (available for all subjects in the whole Sweden). In case of death, hospital and death registries will provide the clinical information, and an informant interviews will be carried out.
The same protocol as for the baseline data collection is used, but the information will concern only the follow-up period. We estimate that both the nurse and medical examination will be reduced to one hour, whereas the length of the psychological assessment will remain unchanged (2 hours).